
We take pride in utilizing evidence-based treatments for a simple reason: they work. Similarly, to best serve our clients and their families, we recognize the importance of data collection, research, and program evaluation. We are committed to gathering outcome data on our clients’ experiences at Elements and beyond. On-going data collection helps us understand what’s working for our clients and how to continue improving.
Each new participant of our program is asked to fill out three questionnaires upon intake, at discharge and then six months and one year after discharge. The following graphics are based on data from these questionnaires.
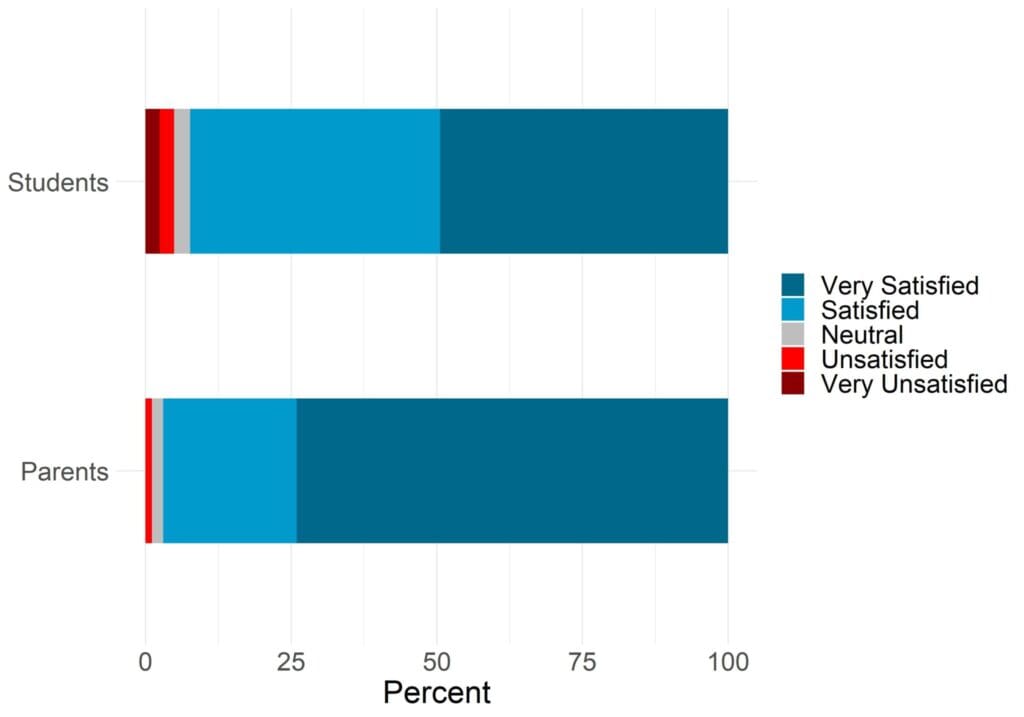
Sample size: Parents = 362, Students = 287
0-1: Very Unsatisfied, 2-4: Unsatisfied, 5: Neutral, 6-8: Satisfied, 9-10: Very Satisfied
97% of Parents and 92% of Students reported being Satisfied or Very Satisfied with their treatment when asked at discharge.
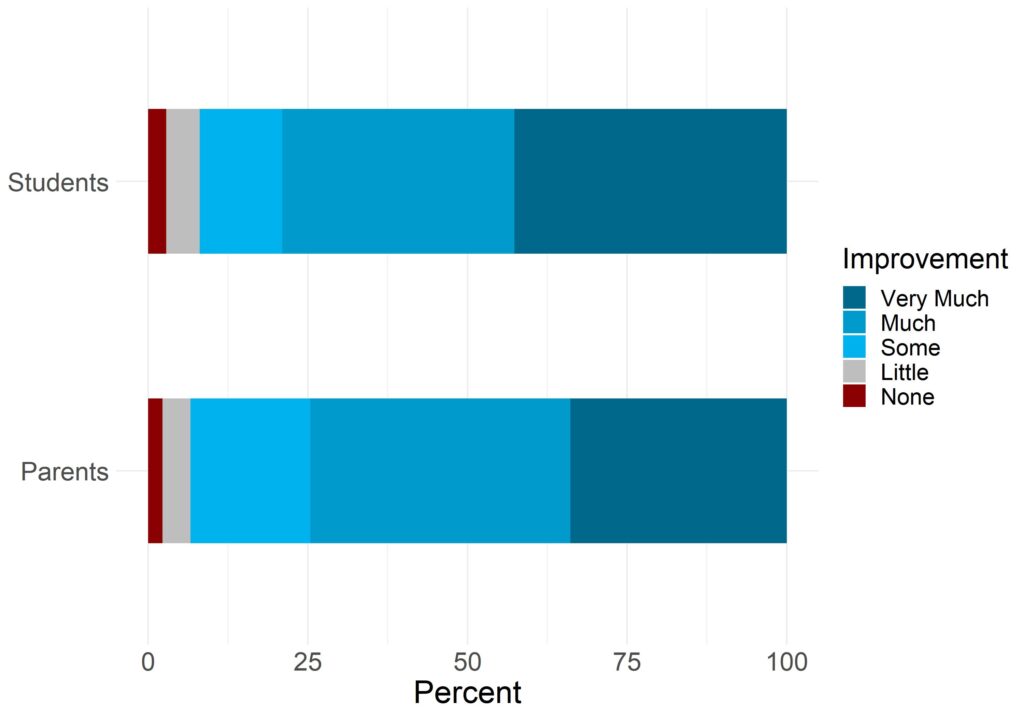
Sample size: Parents = 363, Students = 286
0-1: No Improvement, 2-3 Little Improvement, 4-6: Some Improvement, 7-8 Much Improvement, 9-10: Very Much Improvement
93% of parents and 92% of students reported experiencing between some improvement and very much improvement when asked to rate their or their child’s problems compared to when they entered the program.
At Elements Programs, we strive to provide custom treatment plans tailored to the client’s specific needs. Our admissions team will help fit your child with the group that they will be most likely to succeed in. Most of the clients we work with arrive with several co-occurring diagnoses and often the most evident of these is a compulsive disorder such as technology overuse or substance abuse. These compulsions are almost always just the tip of the iceberg as shown on the following graphics based on Element’s data. Our program focuses on addressing these underlying the root issues an individual is struggling with instead of just the surface level behavioral issues.

Elements focuses on addressing the underlying root emotional causes of maladaptive behavior
Many researchers have documented that exposure to nature can have positive effects on mental health.* The growing field of Outdoor Behavioral Healthcare attempts to unite the intrinsically healing power of nature with clinically tested therapeutic techniques. Elements Programs is based around 6 Core Therapeutic Methods:
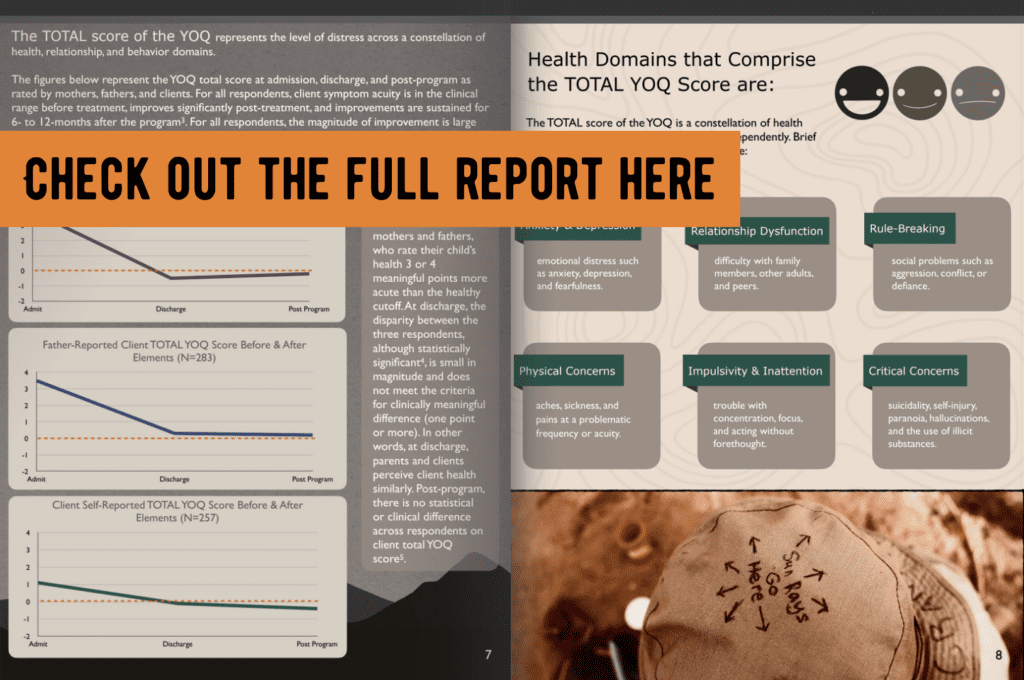
Elements has always pursued the goal of providing cutting edge mental health treatment in a wilderness setting. This treatment equates to improved functioning for our graduates in all areas of life including school performance, family cohesion and peer to peer interaction. In order to provide the best care possible to your child, we utilize a standardized clinical outcome instrument called the Youth Outcomes Questionnaire (YOQ). Click here for more information on the YOQ. The YOQ is used to measure treatment progress in youth populations receiving a mental health intervention.*
MOTHER – REPORTED CLIENT HEALTH
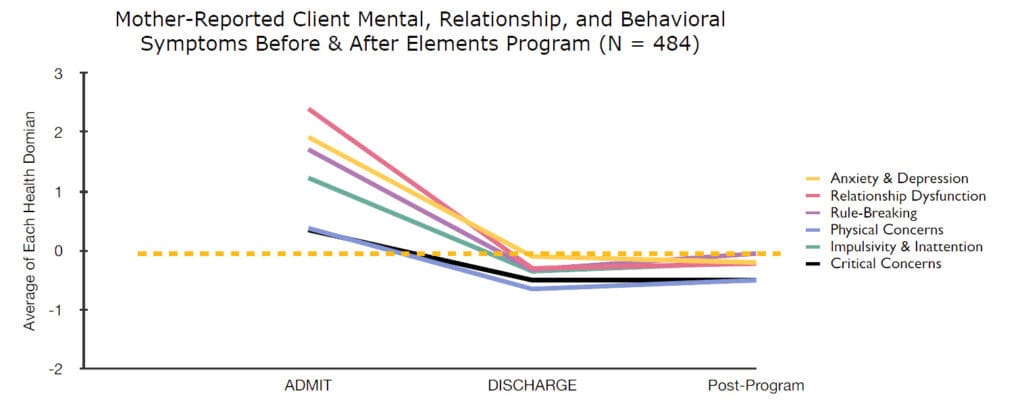
All domains of health were, as reported by 484 mothers, in the clinically problematic range. Notably, Relationship Dysfunction was more than 2 meaningful points less healthy than the cut-off. All YOQ health domains improved into the healthy range at discharge. Treatment gains were sustained up to one year post-program. For all health domains, the amount of change was statistically significant and the magnitude of change was large.
FATHER – REPORTED CLIENT HEALTH
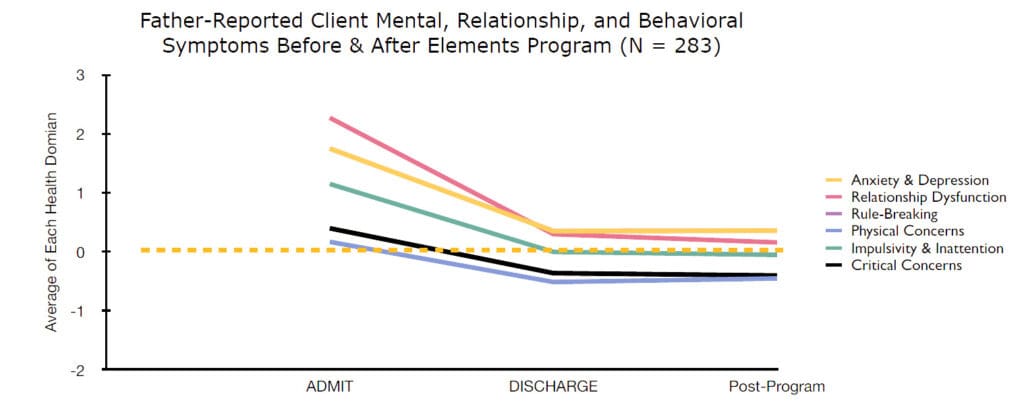
Father-reported client health also indicated clinically problematic health at the time of client admission, and scores improved significantly at discharge. Treatment gains were sustained up to one year post-program. Health changes were statistically significant and the magnitude of change was large for all health domains. On two health domains (physical and critical concerns), the admission scores were close to the cutoff. The improvement on these domains was statistically significant but did not reach the threshold for clinically meaningful change.
Notably, father-rated post-program health was slightly above the healthy cutoff benchmark for three of the health domains: anxiety/depression, relationship dysfunction, rule-breaking.
CLIENT SELF – REPORTED HEALTH
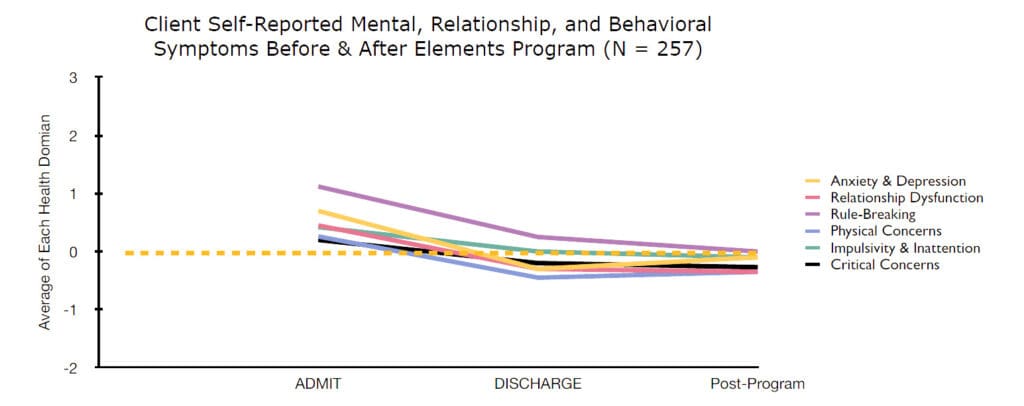
Client self-reports are different from parent reports. Specifically, clients report as healthier than parent reports at the time of admission for most health domains.
Client self-reported improvement is statistically significant, and the gains are sustained for at least a year post-program. The magnitude of change is smaller for clients than their parents, but still large for all but Physical Concerns, where the magnitude of change is .12, or moderate, in size.
General Family Functioning is conceptualized as a family’s capacity to be accepting and collaborative. This capacity is measured with a survey that is called the McMaster Family Assessment Device – General Family Functioning Subscales (FAD-GF). It’s a brief self-report survey that clients and parents complete before, at the end of, and after the program.
Interpreting the results of the FAD-GF is like the YOQ, above. Zero represents the cut-off between healthy and unhealthy family functioning and a change (or difference) of 1 is clinically and statistically meaningful. The FAD-GF is also a symptom scale, so higher scores suggest higher dysfunction; decreases indicate improvement in family functioning.
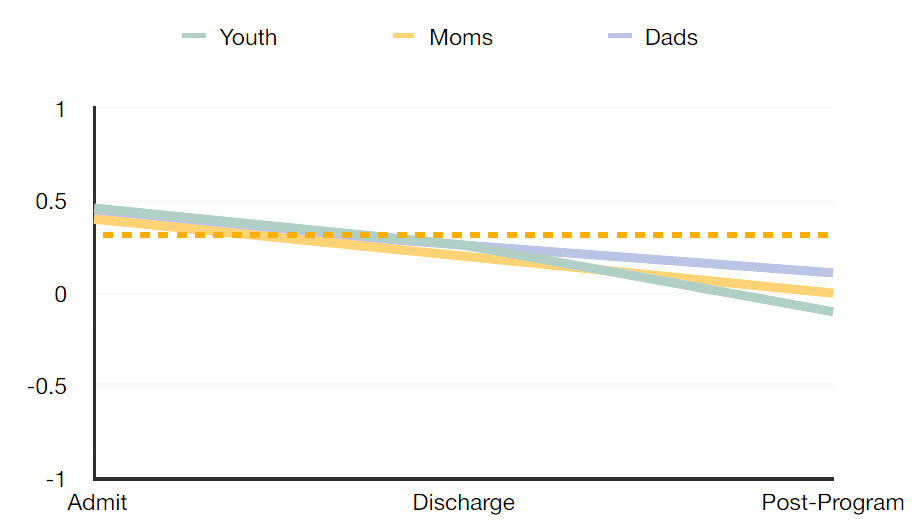
This figure depicts change in family functioning for clients, mothers, and fathers. For each respondent, scores were matched across the three times. As can be seen, family functioning improves, as reported by clients and parents. This change is statistically significant in all three groups, and has a large magnitude of change for clients (moderate for moms and dads). The change does not meet the clinically significant benchmark of 1 unit; however, families tend to move from dysfunctional range (above 0) into or close to the functional cut-off of 0 or less.
Bratman, G., Hamilton, J., & Daily, G. (2012) The impacts of nature experience on human cognitive function and mental health. annals of the New York Academy of Sciences, 1249, 118-136. http://willsull.net/resources/BratmanHamiltonDaily2012.pdf
Burlingame, G., Cox, J., Wells, G., Latkowski, M., Justice, D., Carter, C., & Lambert, M. (2005). The administration and scoring manual of the Youth Outcome Questionnaire. Salt Lake City, Utah: OQ Measures
Gillis, H. L., Speelman, E., Linville, N., Bailey, E., Kalle, A., Oglesbee, N., Sandlin, J., Thompson, L., & Jensen, J. (2016). Meta-analysis of treatment outcomes measured by the y-oq and y-oq-sr comparing wilderness and non-wilderness treatment programs. Child & Youth Care Forum, 45(6), 851–863. https://doi.org/10.1007/s10566-016-9360-3
Tillmann S., Tobin D., Avison W., & Gilliland, J. (2018) Mental health benefits of interactions with nature in children and teenagers: a systematic review. Journal of Epidemiology & Community Health 72(10), 958-966.
**Note: all data presented contains some percentage of predicted values based on a linear model. No difference was found statistically between these predicted values and the original data.
Copyright © 2024 Elements

 (866) 542-2252
(866) 542-2252